HOW TO KEEP GROWTH PLATES OPEN – DELAY THEIR CLOSURE
Is there a way to re-open growth plates after adulthood?
How Do you keep them open or stop them from growing?
Can you re open them?
Can you still grow taller if your growth plates are closed?
These are some of the common questions asked by teenagers whose growth window is still open but closing soon and this article will address them accordingly.
First, bones don’t just grow longer; they grow long after a rapid production chondrocytes (cartilage cells) in the growth plates of the long bones.
So what needs to be done?
If you are still in puberty stage or your growth are still open, you need to take full advantage of this growth window before its shut down.
In this guide, I’ll walk you through how cartilage cells actually build new bone, how to check where you stand with your growth right now, and what determines when your growth plates finally close.
what exactly are growth plates?
Simply put, the epiphyseal / growth plates are thin layers of cartilage disc entrapped at the distal ends of long bones between the epiphysis (head ) and metaphysis .
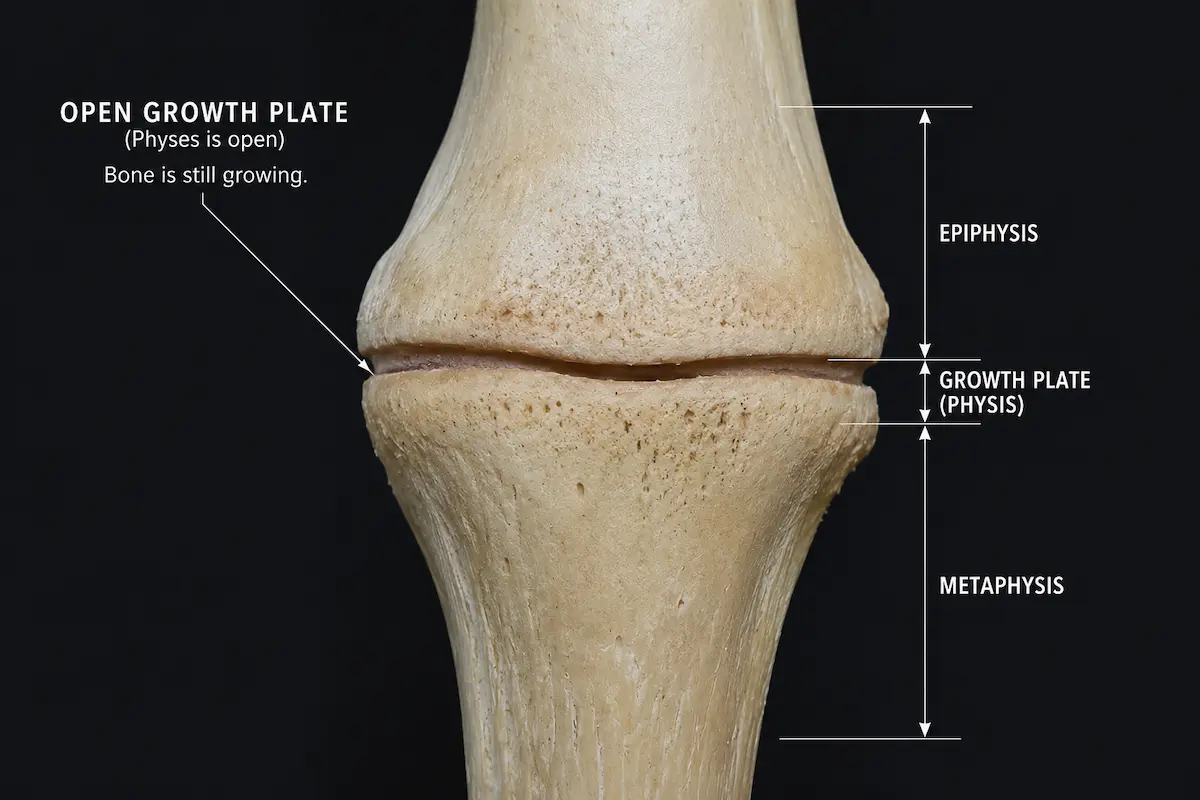
There’re two growth plates in all long bones with one located at each end of the long bone.
Which Bones Have Growth Plates in Human Body?
Like earlier mentioned, growth plates are located in long bones. Examples include:
· The femur (thighbone) · The tibia and fibula (shin bones) · The radius and ulna (forearm bones) · The metacarpal bones in the hands· The vertebrae (back bones) · The humerus (upper arm bone)
What Exactly Is the Growth Plate Made Of ?
A growth plate is not a uniform slab of cartilage.
It is made up of three distinct functional zones, each with a specific role in bone lengthening:
1. The Resting Zone (Reserve Zone)
This is the outermost zone, closest to the epiphysis.
Inside the growth plate cartilage are small, scattered cartilage cells that can multiply and eventually become new bone.
In most cases, these cells are dormant, but that’s where the cells for the the next layer come from.
Without a healthy resting zone, the entire growth process breaks down.
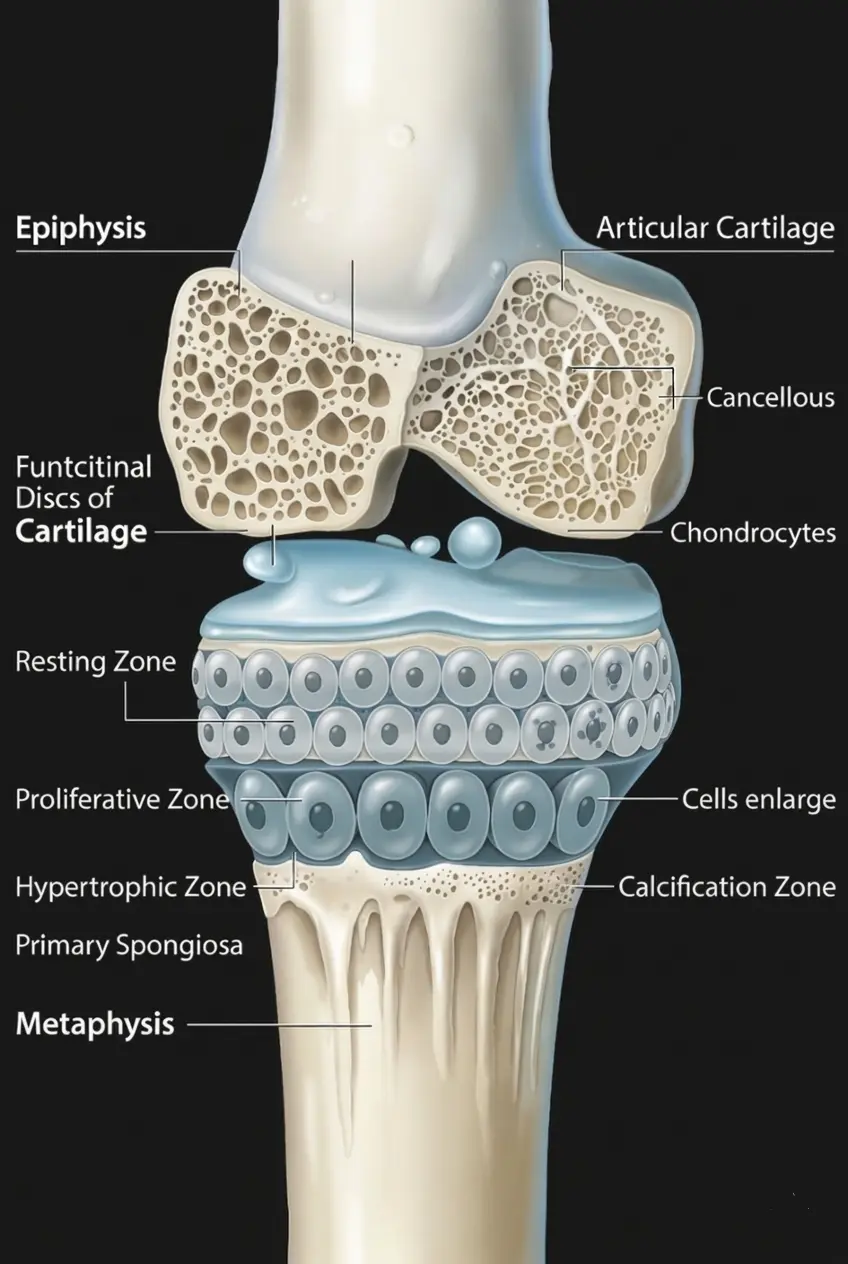
2. The Zone of proliferation.
This is where bone growth originates.
Chondrocytes (bone cells) in this zone multiply fast and line up in neat columns just like a stack of coins..
This zone is the most metabolically active and has the most extensive blood supply, which allows nutrients and hormones (particularly Growth Hormone and IGF-1) to reach their targets efficiently.
The rapid cell division in this zone is what physically pushes the ends of the bone apart, creating length.
3. The Hypertrophic Zone
In this zone, chondrocytes enlarge dramatically , sometimes up to 10 times their original size and begin producing Type X collagen and alkaline phosphatase.
This sets up the cartilage matrix for hardening.
After the chondrocytes accomplish their role, they die off.
A process known as apoptosis .
Calcium and phosphorus are then deposited to harden what’s left into solid bone.
Note: Understanding these three zones is important because disruptions in any one of them , whether from hormonal imbalance, injury, or nutritional deficiency can directly impair height potential.
The Science of Bone Lengthening: How Growth Occurs at the growth Plate.
Bones grow through a cellular manufacturing process called endochondral ossification.
This is how it works step by step :
Stage 1: In the zone of proliferation, immature cartilage cells (chondrocytes) multiply rapidly, creating a scaffolding of new cartilage tissue.
Stage 2: These cells grow larger and produce a structural matrix template which acts as the foundation for forming new bone.
Stage 3: As As the older cartilage cells die off, calcium and phosphorus are deposited to start hardening the space they left behind.
Stage 4: Once the matrix hardens into solid bone tissue, the bone grows slightly .
This process continues and bone keeps growing longer until the cartilage is entirely replaced by solid bone a state known as epiphyseal fusion. [1]
For details on how bone growth is mediated in the growth plate zone, visit how long bones grow.
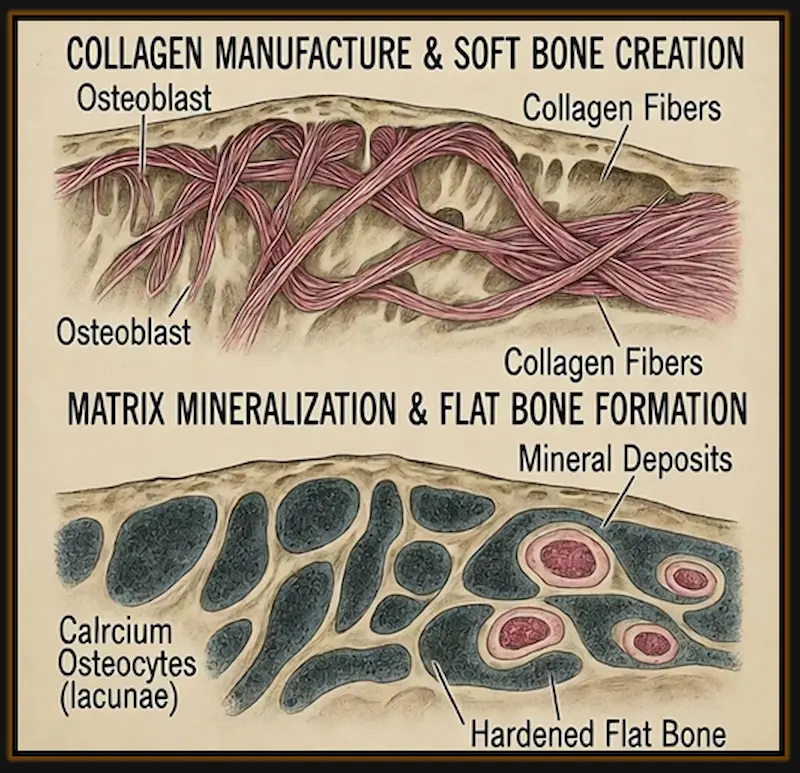
How about Flat Bones? How do they grow?
Flat bones like the skull don’t grow from the cartilage..
They are rather structured by osteoblasts as they develop.
Osteoblasts are the cells that make bone by producing a matrix that then becomes mineralized.
Cells in bones of the skull modify to become osteoblasts.
The osteoblasts then manufacture collagen and create soft bone which is broken down by osteoblasts to manufacture the flat bones.[2]
When Do Your Growth Plates Close or Fuse?
This varies from person to person.
However, according Dr. Andre C. Grant, MD an orthopaedic surgeon at Duke Orthopaedics of Raleigh, most children stop growing approximately 2 years from end of pubertal growth spurt which normally ends at age 14 for girls and 16-17 years for boys.
This means that in most cases, growth plates close between 14 and 16 years for girls and between 16 and 19 years for boys.
In case of Precocious puberty where the child transforms to an adult earlier than expected, the growth plate closes earlier leading to short stature.
| Category | Girls | Boys |
|---|---|---|
| Pubertal growth spurt ends | ~14 years | ~16–17 years |
| Typical growth plate fusion | 14–16 years | 16–19 years |
| Precocious puberty threshold | Before 8 years | Before 9 years |
What About Precocious Puberty?
In cases of precocious puberty , where a child transitions to adulthood earlier than expected, growth plates close prematurely, often leading to shorter adult stature.
If a girl enters puberty before 8 years or if a boy enters puberty before 9 years, then that’s referred to as Precocious puberty.[6]
Important Caveat:
The entire process of growth plate closure in humans is not fully known since what is known is based on animal studies yet majority of animals don’t have much in common with humans.
Rodents have some degree of correspondence with humans but their growth plates don’t fuse at the end of puberty.[7]
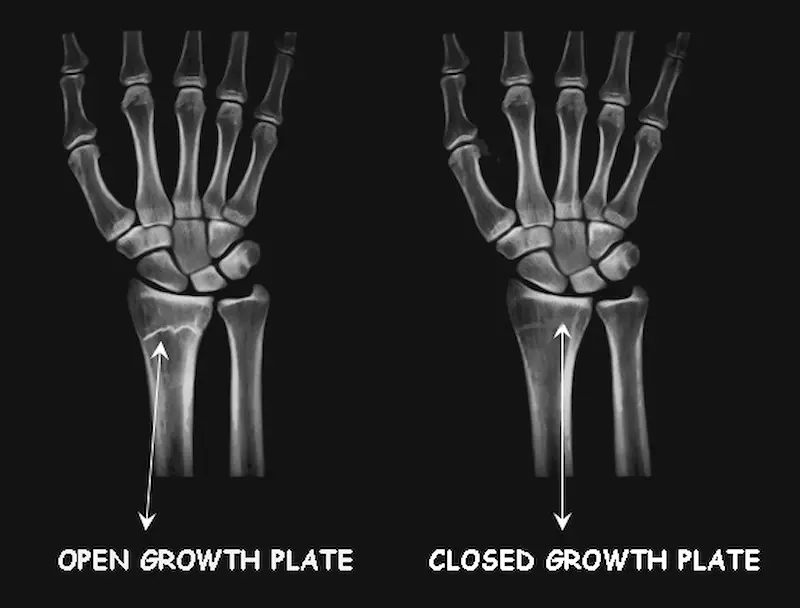
How to check if Growth Plates are closed or still open.
Growth plate status cannot be determined at home.
X-ray scans must be performed by a medical professional in a clinical setting to accurately assess skeletal maturity.
What the Doctor Does
A doctor will look for a visible gap at the ends of the bones.
A visible line means the plate is open; a solid bone connection means it has fused.
X – ray Showing Open Vs Closed Growth Plates.
The Greulich-Pyle Method
The standard tool used by physicians is the Greulich-Pyle Atlas.
A doctor compares an X-ray of your left hand and wrist against this established atlas of maturity markers. This allows them to determine whether your skeleton is maturing faster or slower than your chronological age, a concept known as bone age.
Again, X-ray scans must be performed by a medical professional in a clinical setting to accurately assess skeletal maturity not at home.
[Read the Full Guide: How Bone Age is Assessed using the Greulich-Pyle Method »
The Hormonal Control of Growth Plate Activity.
The timing and rate of growth plate activity is primarily regulated by two hormonal systems — one that accelerates growth and one that brings it to a close.
Growth Hormone (GH) and IGF-1: The Accelerators
Growth Hormone, produced by the pituitary gland, is the primary driver of longitudinal bone growth.
However, GH does not act directly on the growth plate in all cases.
Much of its effect works through Insulin-like Growth Factor 1 (IGF-1), which is mainly produced by the liver in response to GH secretion.
IGF-1 acts directly on chondrocytes in the growth plate zone of proliferation, thereby stimulating cell division and matrix production.
It also controls how fast those cells mature, by speeding some stages up and slowing others down. [3]
It’s why children with growth hormone deficiency end up being much shorter if the condition isn’t treated, and growth hormone therapy works, but only while the growth plates are still open.
Estrogen and Estradiol: The Biological Brake
While Growth Hormone acts as the catalyst for bone growth, estrogen is the one the stops the growth.
Estrogen is secreted among both males and females, particularly in the form of estradiol.
Estrogen accelerates the depletion of progenitor cells in the growth plate’s resting zone, progressively shutting down the cellular engine of bone growth. [4]
Because the secretion of estrogen significantly increases in girls during puberty, girls tend to stop growing earlier than boys.
Evidence from animal research:
This mechanism was confirmed in an experiment where rabbits were inoculated with estradiol cypionate for 5 weeks.
The treatment significantly reduced both the height of the growth plate cartilage and the number of reproductive cartilage cells. [5]
The Three Natural Estrogens.
The body produces three naturally occurring estrogens:
- Estradiol : ls the most predominant estrogen out of the three naturally occurring estrogens produced in the body.The main role of estradiol is to regulate the female menstrual cycles and reproductive system as well as development of sexual features like widening of hips and breast development.[8]
Among males, estradiol regulates sexual desire, sperm production and erectile function.
- Estrone : A weaker estrogen, mainly secreted by fats cells and adrenal glands.
It’s the dominant hormone after menopause.
- Estriol: The weakest form of estrogen, mainly secreted during pregnancy and after birth.
It is also used to treat virginal dryness.
The Role of Nutrition in Growth Plate Health.
Nutrition has a direct impact on how efficiently growth plates function.
Deficiencies in key nutrients can impair chondrocyte activity, reduce bone mineral density, and in some cases accelerate premature closure.
| Nutrient | Role in Bone Growth | Deficiency Effect |
|---|---|---|
| Calcium | The main mineral your bones need to harden. It is critical during the final stages of growth plate activity. | weaker bones due to poor bone mineralization. |
| Vitamin D | Helps your gut to absorb calcium and keeps growth plate cells functioning properly. | Rickets in children or soft, poorly mineralized bones |
| Protein | Supplies the amino acids your body needs to build collagen and cartilage. | Lower IGF-1 levels leading to stunted growth. |
| Zinc | Needed for cell division inside the growth plate. | Slows cartilage cell production and stunts growth . |
| Vitamin A | Controls how bone building and cartilage cells development. | Too much Vitamin A can cause growth plates to close early. [9] |
| Vitamin K2 | Activates the protein that directs calcium into bone instead of soft tissue. | Calcium doesn’t get used properly in the bone. |
The Role of Exercise and Mechanical Loading
The growth plate does not operate in a hormonal vacuum.
physical forces placed on the skeleton also influence how bones grow and develop.
This is known as bone mechanotransduction: the process by which bone cells convert external physical forces exercise, and tension into signals, that regulate bone remodeling, repair, and density.
How does Exercise Affect The Growth Plates?
The physical for applied to bones during exercise is one of several important factors that influence bone growth.
The others include genetics, hormonal levels, the and your nutritional status.
Moderate, weight bearing activities trigger growth plate cells and promote the release of both Growth Hormone and IGF-1.
Research shows that Physical activities like jumping, running, and resistance training support healthy bone development.
what causes growth plates to close?
It is understood that as puberty progresses, the production of new chondrocytes in the resting and proliferative zones can no longer keep pace with the rate of ossification in the hypertrophic zone.
Essentially, the cellular engine slows down until the growth plate is entirely replaced by solid bone, a state called epiphyseal fusion.
The primary driver of this process is the hormonal surge of estradiol toward the end of puberty, which accelerates the depletion of progenitor cells and ultimately brings the growth process to a close in both sexes.
How to prevent growth plates from closing if you are still in puberty (how to keep them open naturally)
If you are still in puberty stage, your goal is likely to keep growth plates active as long as possible.
Several interventions ranging from natural compounds to pharmaceutical agents have been studied for their ability to slow skeletal maturation.
1. Resveratrol supplementation
Resveratrol is a polyphenol compound produced by certain plants when attacked by pathogens or physical injury.
It is found naturally in red grapes, blueberries, and peanuts, and is widely available as a dietary supplement.
In a study using pre-pubertal female rabbits (chosen because their growth plate fusion timing mirrors that of humans), resveratrol treatment improved longitudinal bone growth and significantly delayed growth plate closure.
The impact on enhanced long bone growth was attributed to the delay in growth plate fusion, resulting in greater final bone length. [10]
It’s likely that resveratrol exerts this effect partly because it contains anti estrogenic properties.
By regulating the effects of estrogen, it may slow down the depletion of growth plate cells due caused by estradiol.
2.Tamoxifen (Nolvadex)
A drug used to treat the enlargement or swelling of breasts among men.
This condition is normally a result of too much secretion of estrogen hormone compared to testosterone in men.
Estrogen is a female sex hormone responsible for development of sexual and reproductive features in women breasts inclusive.
Tamoxifen is also used to treat breast cancer in both men and women.
When short teenage boys who were still in puberty with an average age of 14 – 15 years were administered with 10 – 20mg of tamoxifen twice everyday for an average of 26 months, their skeletal bones matured very slowly which slowed down the closure of their growth plates thus increasing their predicted adult height average by approximately 10 cm.[11]
Note: Tamoxifen is a prescription medication with potential side effects.
It should only be used under direct medical supervision.
This information is provided for educational purposes only.
3. Aromatase inhibitors.
Aromatase is an enzyme responsible for estrogen synthesis by converting androgens to estrogen.
Androgens are hormones responsible for male characteristics.
For instance testosterone.
Aromatase inhibitors are drugs that hinder the secretion of estrogen hormone.
They are also used to treat cancer among older women.
such drugs include Letrozole, Aomasin and Arimidex.
When puberty ends, male and female reproductive glands secrete estrogen hormone in higher quantities.
Estrogen then speeds up the process of growth plates closure.
Thus, since aromatase inhibitors inhibit estrogen production, closure of growth plates will be delayed by the drugs
Commonly used aromatase inhibitors in clinical research include:
- Letrozole
- Exemestane (Aromasin)
- Anastrozole (Arimidex)
Aromatase inhibitors are also used to treat estrogen-receptor-positive cancers in post-menopausal women.
In the context of bone growth, their use in adolescent boys with short stature has shown meaningful increases in predicted adult height in several studies. [12]
Note: Aromatase inhibitors are potent pharmaceutical agents with significant systemic effects.
They should only be considered under careful endocrinological supervision.
Self-administration is strongly discouraged.
4. GnRH Analogs and CNP Analogs
Two additional therapeutic interventions have been studied for their potential to delay growth plate closure:
a) Gonadotropin-Releasing Hormone (GnRH) Analogs:
Normally, the brain sends a pulsing signal called GnRH (Gonadotropin-Releasing Hormone) to tell the body to produce hormones like estrogen or testosterone.
Hence, GnRH analogues are man-made drugs that “mimic” or block that signal to change how much hormone your body makes.
GnRH analogs work by suppressing the pituitary gland’s secretion of LH and FSH, the hormones that trigger puberty and the subsequent rise in estradiol.
By delaying the hormonal cascade of puberty, GnRH analogs effectively extend the window of growth plate activity.
They are currently used clinically in cases of precocious puberty to slow premature sexual development and preserve height potential. [13]
b) C-Type Natriuretic Peptide (CNP) Analogs:
CNP is a peptide produced locally within the growth plate that stimulates chondrocyte proliferation and matrix production.
Recombinant CNP analogs (such as vosoritide) are recognized for their ability to promote longitudinal bone growth and may delay growth plate closure.
They are currently used or studied as treatments for achondroplasia, a form of dwarfism caused by a mutation that impairs growth plate function.[14]
Frequently Asked Questions
1. What are the signs that growth plates are closing?
The only real way to know is an X-ray, usually of the left hand and wrist, read against the Greulich-Pyle atlas I mentioned above.
That said, there are a few clues you can notice like height gain slowing down to almost nothing in over 6 to 12 months is usually the first hint.
Shoe size staying the same for a year or more is another one people tend to bring up a lot.
Full facial and body maturity, or looking like a fully grown adult at a young age is another sign.
2. How do you stimulate growth plates?
When they’re still open, the growth plate responds to two main things : hormones and mechanical load.
On the hormone side, Growth Hormone and IGF-1 are what push chondrocytes to divide at the zone of proliferation, which is why deep sleep matters so much, that’s when most of your GH gets released.
On the mechanical side, moderate weight bearing activities like jumping, running, and resistance workouts sends a signal through the bones that supports healthy plate activity, this is the mechanotransduction process discussed earlier.
Nutrition ties both of those together. Calcium, vitamin D, protein, zinc, and vitamin K2 all play a direct role, and being short on any of them slows the whole process down, sometimes without you noticing until growth stalls.
3. What causes growth plates to close early?
The main driver is estrogen, and this applies to both sexes.
Like earlier mentioned, as puberty winds down, estradiol rises and starts depleting the resting zone of the growth plate faster than it can be replaced.
4. Can growth plates reopen?
No, not once they’ve fully fused.
The cartilage gets replaced by solid bone through the ossification process and that’s permanent.
A note for those whose plates have already closed:
Everything covered on this page assumes the growth plates are still active. If yours have fused or you suspect that you have delayed bone age, the mechanics shift significantly.
The focus moves from preserving plate activity to applying targeted mechanical load directly to the bone and periosteum through specific exercise sequencing and recovery timing to increase your chances of height increase.
Reading Recomendation
The Grow Taller After Puberty Exercise Routine Handbook
References And Further Reading
1. Developmental Biology, 6th Edition (2000)
2. The Emergence of Bone (2000)
3. Longitudinal Bone Growth and the Growth Plate (2020)
4. Cellular and Molecular Mechanisms of Estrogen-Mediated Growth Plate Fusion (2014)
5. Evidence That Estrogen Hastens Epiphyseal Fusion and Cessation of Longitudinal Bone Growth by Irreversibly Depleting the Number of Resting Zone Progenitor Cells in Female Rabbits (2002)
6. Physiology, Bone (2023)
7. Growth Plate Senescence and Catch-up Growth (2011)
8. Estradiol (2023)
9. Cellular and Molecular Mechanisms of Estrogen (2014)
10. Resveratrol Treatment Delays Growth Plate Fusion and Improves Bone Growth in Female Rabbits (2013)
11. Cellular and Molecular Mechanisms of Estrogen-Mediated Growth Plate Fusion (2014)
12. Height Increment and Laboratory Profile of Boys Treated With Aromatase Inhibitors With or Without Growth Hormone (2017)
13. The Gonadotropin-Releasing Hormone Analogue Therapy May Not Impact Final Height in Precocious Puberty of Girls With Onset of Puberty Aged 6 – 8 Years (2019)
14. Assessment of the efficacy of vosoritide therapy in children with achondroplasia in clinical trials (2024)
Watch, stories of acromegaly patients who continued growing in 20
s 30s 40s and 20s
AUTHOR BIO

Dennis Raney (B.Sc.) is an author and a blogger specializing in natural body growth optimization strategies.
After years of navigating the psychological and physical challenges of being under-average height, Dennis dedicated over a decade to researching the intersection of lifestyle, nutrition, and body growth.
By applying an evidence-based approach to healthy lifestyle changes, he successfully navigated his own body transformation, an experience that led him to author his comprehensive guide on height increase during and after puberty.
Today, he shares practical, research-backed strategies through his book and blog to help others overcome similar challenges.”
Interested in connecting? :
✉️ Send an email: Dennis »»
💬 Add me on Discord: raney0029 »»
RELATED POST :